


Objective
To investigate the effectiveness of MANUAL’s complete testosterone replacement therapy (TRT) treatment service for men with low testosterone (hypogonadism).
Introduction
In an era marked by a progressively ageing population and a surge in chronic diseases, the prevalence of low testosterone (also known as an androgen deficiency) has steadily risen over the past few decades, signalling a crucial health concern1.
What is testosterone?
Testosterone is a powerhouse hormone responsible for the development of traditionally masculine traits, from deepening voices to the growth of body hair, enlarged skulls and bones, enhanced muscle size and strength, heightened sexual libido, and a sense of “manliness”1.
Beyond its role in physical attributes, testosterone plays a pivotal role in the health of both men and women including in cardiovascular health, energy production, resilience (both physical and psychological), and the proper functioning of the nervous and immune systems.
Learn more about testosterone here.
Is there a relationship between testosterone and aggression? Find out here.
What are symptoms of low testosterone?
The repercussions of dwindling testosterone levels can manifest in a myriad of symptoms including: erectile dysfunction, decreased libido, fewer spontaneous erections, sleep disturbances, depression, low self-confidence, fatigue, and cognitive impairment2.
Uncover details about signs of low testosterone here.
Do some foods lower testosterone levels? Learn about it here.
Do Brazil nuts increase testosterone levels? Find out here.
Need tips (including what foods to eat) to increase testosterone? Discover more here and here.
Why should I care?
Studies have found that low testosterone is not only affecting older men; 40% of men over 45 years old, and 50% of those in their 80s grapple with low testosterone levels3 4, which gradually decline with age (roughly 1.5% per year for total testosterone and 2-3% per year for free testosterone)5 6.
This decline in testosterone levels not only deeply affects one’s overall health and well-being, it also leads to increased risk of various health complications like cardiovascular disease7, Type II Diabetes8 and osteoporosis9 and reduced overall quality of life.
Men with low testosterone are also subject to potential misdiagnoses, ranging from chronic fatigue to depression to other chronic disorders, which further complicate their health journey and delay the appropriate treatment they need.
Learn more about ‘normal’ testosterone levels by age here.
What can I do? What is TRT?
Testosterone Replacement Therapy (TRT) can be a life-changing intervention that restores testosterone levels to their optimal range in as little as 3 weeks.
TRT is a personalised medical treatment that addresses low testosterone by supplementing the body with externally administered testosterone which restore levels to within the normal range. Injections, topical gels or patches, or subcutaneous pellets can be used to administer this.
MANUAL, the leading TRT clinic in the UK, evaluated the impact of MANUAL’s proprietary TRT treatment service over 6 months. The study sought not only to explore the tangible effects on total and free testosterone levels but also to explore the quality of life changes of adult men on TRT treatment.
Get additional details about TRT here and its benefits and side effects here and here.
Methods
We conducted a retrospective cohort analysis among 132 adult male patients of MANUAL in December 2023.
Eligibility
To ensure that TRT was the right fit, potential TRT candidates completed (in the following order):
- A simple at-home finger prick blood test
- Measuring total and free testosterone
- Results received in 48 hours
- A enhanced blood test
- Comprehensive blood test (including liver, kidney, and PSA levels), collected by a nurse
- To confirm initial results, learn more about their health, and assess their safety for TRT treatment
- A comprehensive medical history form (including quality of life assessment–more details below)
- A video consultation with our experienced in-house doctors who specialise in TRT
- Discusses blood test results, treatment options, and monitoring process
Additional criteria based on age:
- 25-50 years old: free testosterone level below 0.225 nmol/l AND a total testosterone level < 15 nmol/l
- < 25 years OR > 50 years old: free testosterone level below 0.225 nmol/l AND a total testosterone level between < 12 nmol/l
What happened next for those eligible for the study?
Doctors prescribed the appropriate injection treatment — testosterone cypionate, enanthate or isocaproate — and simple step-by-step videos for injection training.
Some men received additional therapies:
- On recommendation by the TRT doctor, some received:
- Aromatase inhibitors: for patients with excess body fat or genetic factors causing raised oestrogen levels
- Optional treatment:
- Human chorionic gonadotropin (HCG was used if patients are interested in maintaining their fertility)
Keeping tabs on progress:
We followed up with participants at the 6 week, 3 month, and 6 month mark after starting TRT treatment. At each time point, patients completed blood tests and quality of life assessments of their well-being, including consultations with their doctor to 1) monitor both physical progress (including any side effects) and their overall state of health and 2) make adjustments to the treatment as needed.
Questionnaire
The Androgen Deficiency (low testosterone) in the Aging Male (qADAM) is a validated questionnaire widely used among doctors as a diagnostic tool to evaluate how much low testosterone might be affecting an individual’s life. You can read more about it here.
The questionnaire consists of 10 questions about symptoms of low testosterone, with the participant scoring between 10-50. The lower the score, the more symptoms someone might be dealing with, and the higher the score, the fewer symptoms they may have.
The qADAM questionnaire is a valuable tool that allows MANUAL doctors to understand the unique circumstances of each individual. This understanding enables them to tailor a personalised journey for every person, ensuring they receive the most optimal results and support according to their specific needs.
Results
Demographics
Summary statistics were summarised by means (and standard deviation). At baseline, the mean age of participants was 38.3 (SD 8.9), with nearly half (47%) of patients aged 35-44 years. Mean BMI among participants was 29 kg/m2 (SD 5.0). Subgroup analyses by baseline BMI were also conducted to assess potential differences in individuals with a normal weight range (BMI <25) and overweight/obese individuals (BMI>25).
Effectiveness
Biomarkers
From the start of the survey to 3 months, robust increases were observed in free testosterone levels, with mean levels of 0.2nmol/l at pre-treatment increasing to 0.8nmol/I (mean change: 0.6nmol/I; 312% increase) at 3 months, and further rising to 0.9nmol/I (mean change from baseline: 0.7nmol/l; 324% increase) at 6 months.
Similar observations were reported for total testosterone levels, with mean levels of 10.4nmol/I at the start rising to 30.4nmol/I (mean change: 20nmol/I; 237% increase) at 3 months and 31.3nmol/I (mean change from baseline: 20.9nmol/I; 256% increase) at 6 months.
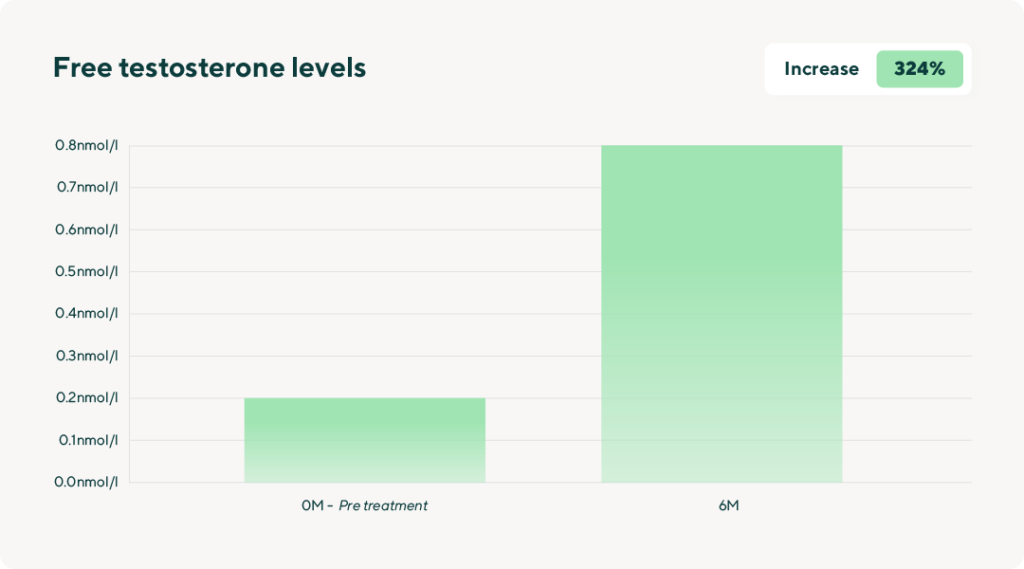
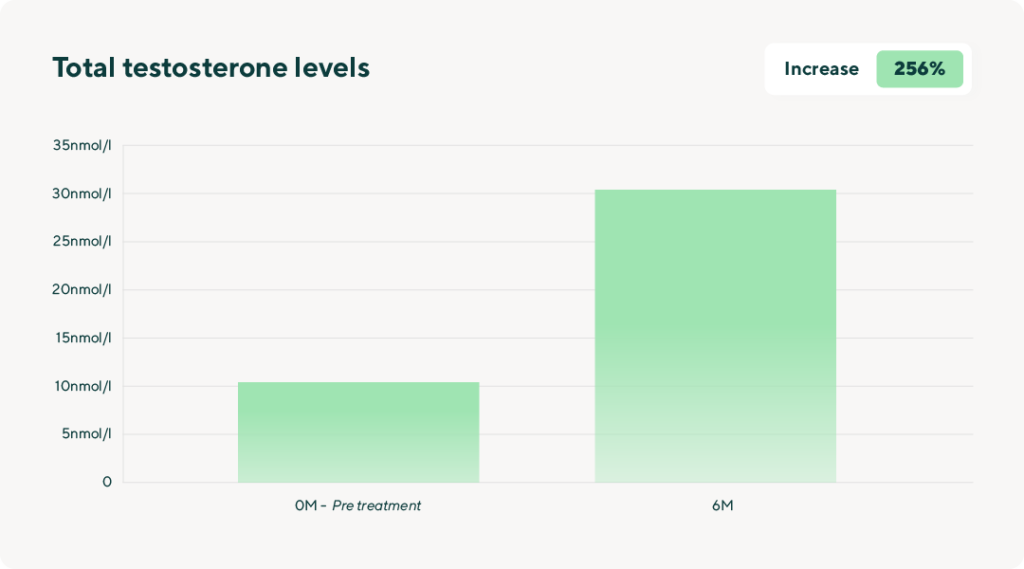
When categorised according to BMI, results were particularly notable among those at a ‘normal’ weight: the mean of their free testosterone levels increased by 0.8nmol/I (495%) at 6-months compared to an increase of 0.6nmol/I (295%) for overweight patients, and mean total testosterone of those at a ‘normal’ weight increasing by 27.8nmol/I (385%), compared to an increase of 19.5nmol/I (235%) increase among overweight patients.
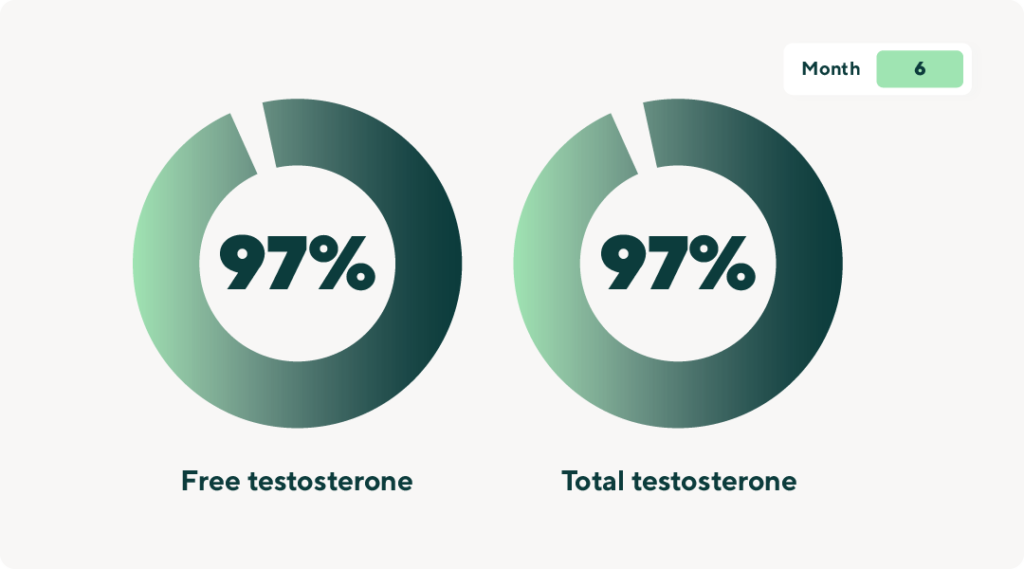
Nearly all patients saw improvements in their free testosterone levels, with 94% experiencing positive changes after 3 months and 97% after 6 months. Similarly, 95% of patients showed enhancements in total testosterone levels after 3 months, increasing to 97% after 6 months. Similar observations were observed when ranked by BMI.
Change in symptoms
Among the 132 patients who completed the questionnaire at 0 and 6-month time points, the mean qADAM score (range: 10-50; 10=most symptomatic, 50=least symptomatic) increased from 25.9 at baseline to 36.6 (mean change: 49.3%; mean rebaselined (weighted score) change: 95.1%) at the 6 month time point.
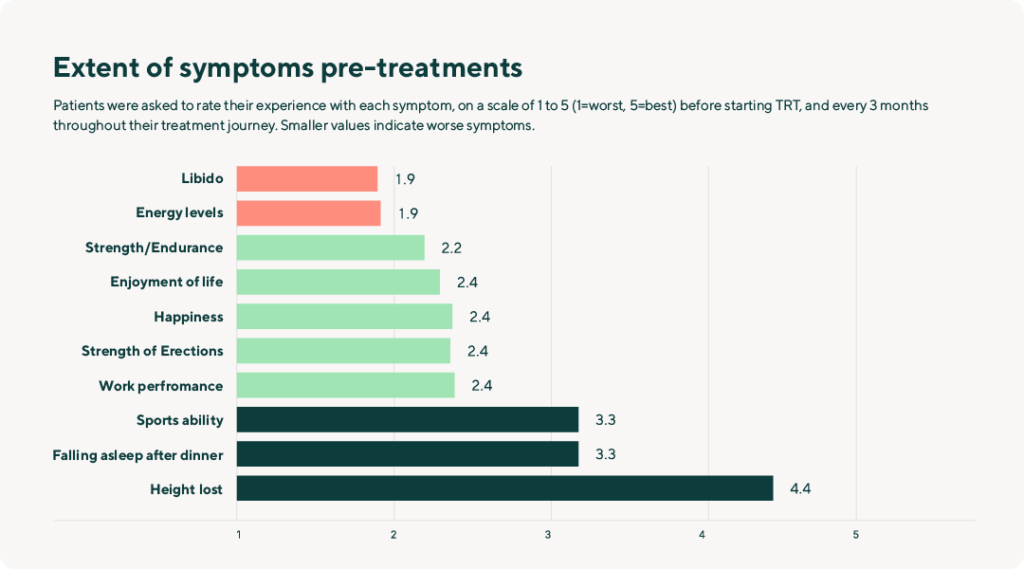
At baseline, the highest concerns of individual symptoms (range: 1-5; 1=worst, 5=never/best) that patients reported were: libido (1.9), energy levels (1.9), and sports ability over the past 4 weeks (2.2).
From baseline to 6 months, the majority (68-86%) of patients reported notable progress across all assessed symptoms patients experienced. Improvements were evident in the energy levels of 86% of patients, 79% in libido, enjoyment of life, and frequency of falling asleep, 76% in sports ability, 75% in happiness, 74% in work performance, 73% in strength, and 68% in erection strength.
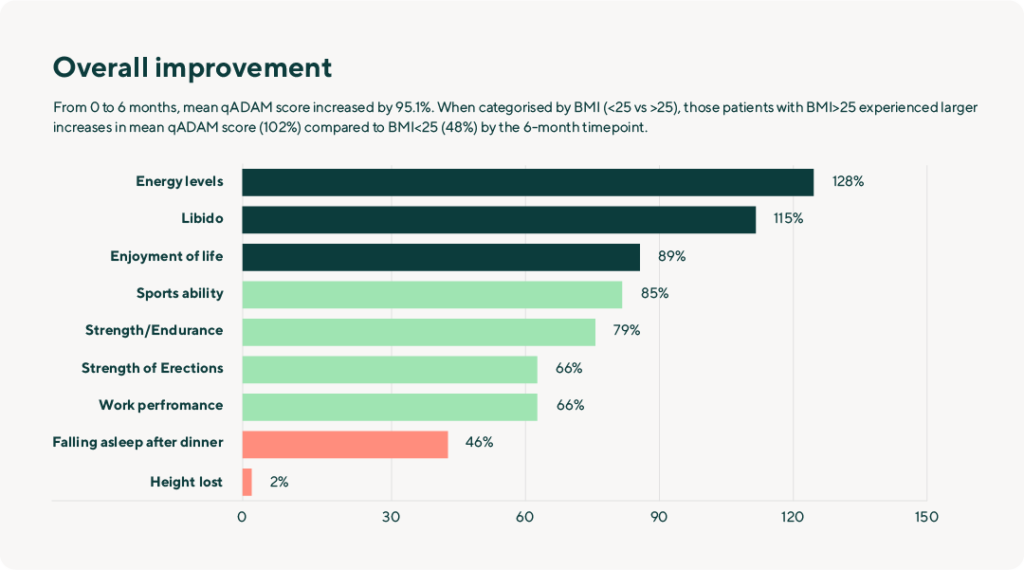
When analysed by symptom, we saw increases in the mean point across all categories over a 6-month period: 1.6 (128%) in energy levels, 1.5 (115%) in libido, 1.3 (89%) in enjoyment of life, 1.3 (85%) in sports ability, 1.3 (79%) in strength, 1.1 (66%) in strength of erections, 1.1 (66%) in work performance, and 0.6 (46%) in frequency of falling asleep.
When categorised by BMI (<25 vs >25), those patients with BMI>25 experienced larger increases in mean qADAM score (102%) compared to BMI<25 (48%) at 6 months. By symptom, while both groups experienced positive changes, those with BMI>25 experienced up to nearly double the change compared to those with BMI<25 in energy (135% vs 75% increase, respectively), strength (84% vs 45%), enjoyment of life (94% vs 54%), erection strength (69% vs 45%), and work performance (69% vs 45%). Interestingly, those with BMI<25 had greater increases in libido change than those with BMI>25 (140% vs 112%).
Summary
After 6 months, an overwhelming majority of patients showed increased levels in biomarkers of low testosterone (via free and total testosterone) as well as substantial improvements across multiple symptoms (via qADAM). Initial signs of improvement began to emerge at the 3-month mark and continued to intensify throughout the entire 6-month period.
One interesting finding we observed when we looked at patients grouped by BMI was that both categories, whether BMI<25 or BMI>25, experienced clinically meaningful changes in biomarkers and symptoms related to quality of life. Notably, individuals with a BMI<25 demonstrated more substantial changes in free and total testosterone, whereas those with a BMI>25 showed greater changes in most aspects of quality of life symptoms. This suggests a nuanced correlation between body mass index and the specific areas of improvement experienced by individuals undergoing testosterone replacement therapy.
These findings were anticipated: the fundamental mechanism of TRT involves administering exogenous testosterone directly into the body, effectively restoring testosterone levels to a more optimal range. The increases in testosterone levels not only alleviate symptoms of low testosterone and increase overall quality of life, but also underscore the potential impact of lifestyle changes alleviating symptoms, which can boost testosterone levels.
These results show the dynamic nature of the treatment response and highlight the importance of considering individual characteristics in optimising therapeutic outcomes.
Discussion
The initial findings from this study will not only contribute to the existing body of knowledge about testosterone replacement therapy, but also provide valuable insights into the management and treatment options for men with low testosterone in the UK. These findings are still evolving; the subsequent phase will involve reporting observations after 12 months and future intervals, to gain further understanding on the long-term effects of TRT. As we discover more about the effectiveness and potential advantages of TRT, it opens up avenues for developing more precise and personalised approaches to patients in order to optimise health and well-being. By expanding our understanding of TRT, we move closer to empowering individuals affected by low testosterone with strategies that are not just effective but uniquely suited to their needs.
We are excited to share that we will be conducting further research in collaboration with top Universities in the UK. If you are interested in participating and gaining early access to findings, please sign up here: research@manual.co. Your involvement could be a vital part of shaping the future of TRT and contributing to advancements in men’s health.


